
25.07.2024
- minute readminutes read
Therapeutic Options For The Management Of Halitosis
To reduce halitosis, it is important to consistently practice good oral hygiene. In fact, although halitosis has multifactorial origins, the vast majority (90%) of cases are related to oral cavity problems such as poor oral hygiene, periodontal disease, tongue coating, food impaction, unclean dentures, faulty restorations, as well as oral carcinomas and throat infections.

Management of halitosis includes simple measures such as instructions for oral hygiene, tongue cleaning, and mouth rinsing.
Given the range of treatment options and the number of substances that can be useful in the management of halitosis, it is helpful to review mechanical, chemical and biochemical options which can be used, either alone or in combination.
Mechanical cleaning of the tongue
The tongue is populated by a large number of microorganisms [1]. Its cleaning should be included in all therapeutic approaches involving halitosis. In fact, whenever there is a thick coating on the tongue, it should be regularly removed.
Tongue cleaning has an immediate positive effect on halitosis as the number of bacteria is superficially reduced while the papillae remain unchanged [2]. The middle and back thirds of the tongue in particular should be cleaned two to three times daily with the help of a specially designed tongue cleaner (for example, GUM® HaliControl® Tongue Cleaner) to limit discomfort. Tongue cleaning should always be part of any treatment.
Chemical deactivation of odour-causing bacteria
Halitosis treatment should not aim to eliminate all bacteria. It is sufficient to prevent the metabolism of odour causing bacteria.
A wide choice of products are available, some more appropriate than others.
Products containing chlorhexidine (CHX) are not indicated, given eradication of all bacteria is not an objective. Long-term or excessive use of chlorhexidine containing oral rinses can result in damage to the oral mucosa, cause discolouration of the teeth and tongue and lead to taste impairments.
Amine fluorides (AmF) and zinc fluoride rinses have a good antibacterial effect, the surface-active AmF is typically well absorbed on all oral cavity surfaces making its action sufficiency well distributed throughout the oral cavity.
Cetyl pyridine chloride (CPC) and essential oils are also known to have a very good antibacterial effect and thus reduce bad breath. They work by promoting adhesion between oil droplets and bacteria, an effect which is improved by the presence of CP [3].
Biochemical enzymatic inhibition
Bacterial metabolism release enzymes, including those that degrade proteins and amino acids. Zinc can act to stop this enzymatic reaction therefore combatting bad breath.
Binding of odour-causing substances
Odour-causing substances such as volatile sulphur compounds (VSCs) can be bound by Cyclodextrin, a cyclic oligosaccharide, which works by enclosing or neutralising the VSCs thus ensuring they no longer smell. Zinc can also help bind sulphur compounds.
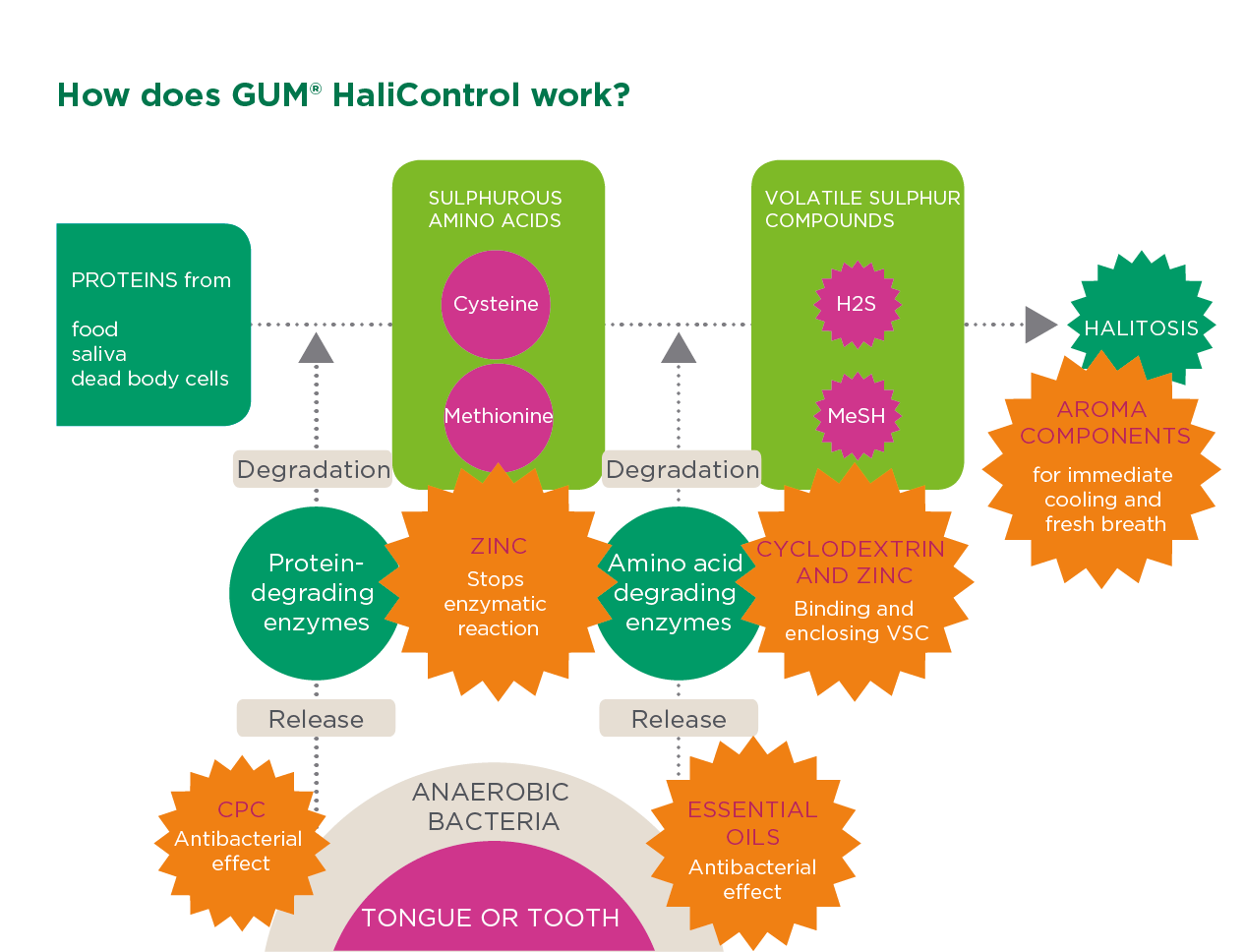
GUM HaliControl combines multiple mechanisms of action to fight halitosis
GUM HaliControl products contain CPC, essential oils, zinc, and cyclodextrin. These substances act in synchrony to neutralize volatile sulphur compounds, inhibit enzyme reactions, eliminate and block odour-causing bacteria, while also providing various aromatic components to produce fresh breath.
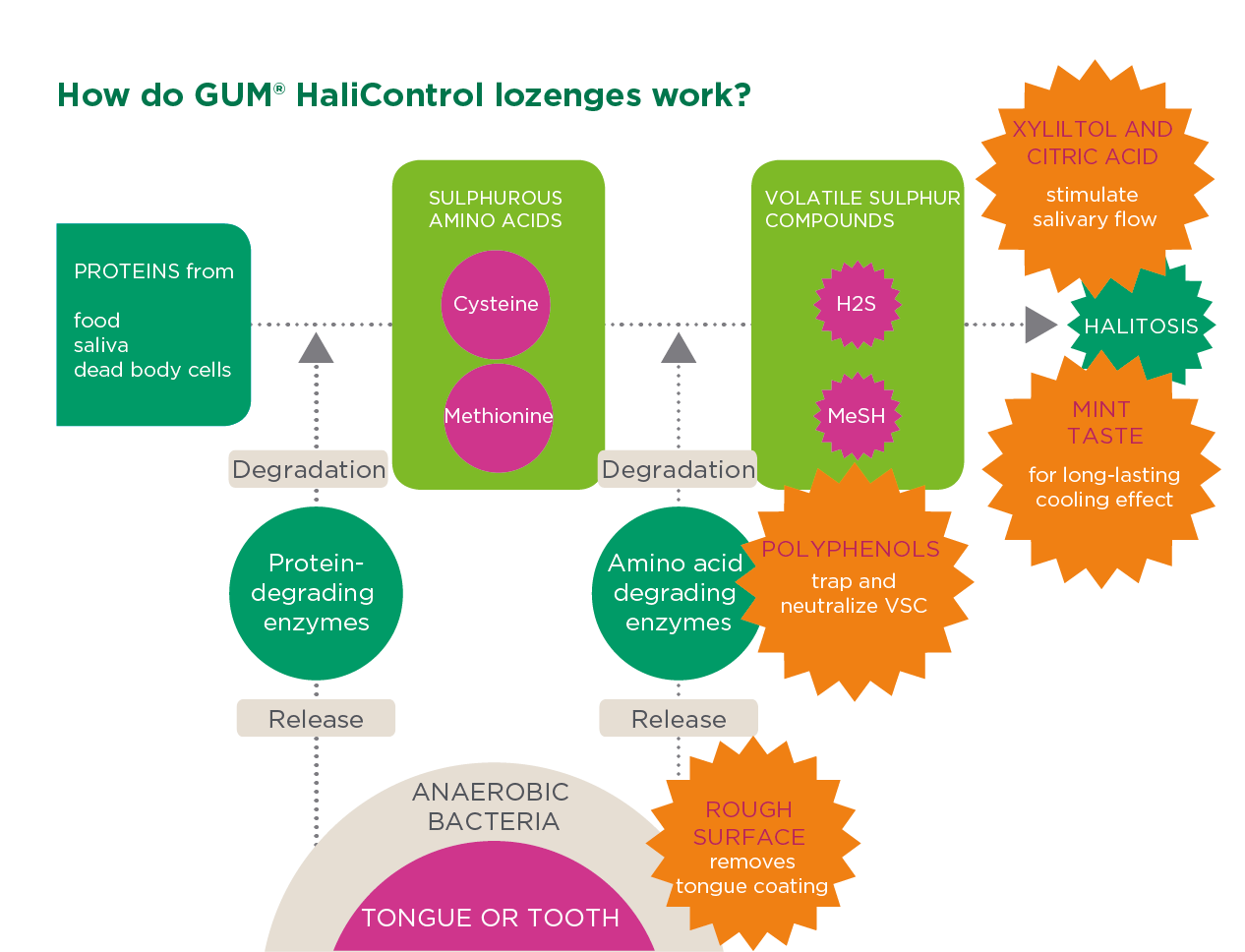
On the go - GUM HaliControl lozenges - A natural approach for temporary halitosis
When it comes to temporary halitosis, such as halitosis caused by food, alcohol and tobacco, GUM HaliControl lozenges with plant-based activated polyphenols can neutralize bad odours and give halitosis sufferers peace of mind.
The surface of GUM HaliControl lozenges acts to reduce tongue coating while the sucking action stimulates saliva production thereby "diluting" odour components and reducing bad breath.
[1] Tonzetich, Joseph. Production and origin of oral malodour: a review of mechanisms and methods of analysis. Journal of periodontology 48.1 (1977): 13-20.
[2] Bordas et. al. Archives of oral biology 53, Suppl. 1 (2008) S13–S18.
Related Articles
-
Probiotics in Pregnancy Hormonal changes during pregnancy can easily lead to gingivitis or periodontitis. Probiotics are a safe and effective adjunct in the management of gum disease.
-
Probiotics and Dentistry: Key Facts and Findings While research into the oral microbiome is ongoing, the early indications about probiotic benefits are as promising as the prospects.

-
Probiotics Reduce Candida Albicans in Elderly Patients Learn about the unique oral health risks faced by older adults, including candidiasis, and the factors contributing to increased susceptibility.
