
13.08.2021
- minute readminutes read
Probiotic Health Maintenance of the Gums
Periodontal diseases arise due to a mismatch between existing pathogenic bacteria and desirable beneficial germs. Of course, the susceptibility of the host also plays a significant role, which is influenced by various circumstances or diseases.

Initial therapy for periodontal diseases focuses on reducing the number of unwanted pathogens through scaling and root planing (SRP).
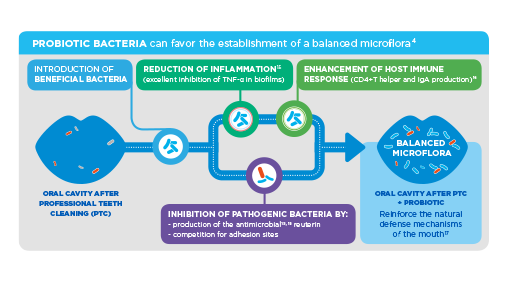
Numerous studies confirm that the probiotic germ Lactobacillus reuteri Prodentis® (LrP) is a useful therapy supplement for periodontal diseases. Studies also show that some bacteria have both antimicrobial and anti-inflammatory properties. The aim of treatment with LrP is to increase the proportion of beneficial bacteria in the oral cavity through probiotics in the long term and to restore the natural balance of the oral flora.
Current study situation
In the study by Teughels et al. [1] 30 patients with chronic periodontitis after performing SRP for 12 weeks received either LrP or placebo. The result shows that the patient group receiving LrP had significantly fewer patients with deep pockets. In addition, a significant reduction of the pocket depth in deep pockets as well as an attachment gain could be determined and also the pathogenic germ Porphyromonas gingivalis was significantly more contained (- 1.17 cfu / ml vs. - 0.22 cfu / ml in the saliva after 12 weeks).
The double-blind study with 30 periodontitis patients by Vivekananda et al. [2] confirms these results. Half of the study participants were treated with one SRP, the other not. From day 21 to 42, one group received two tablets of LrP daily, the other group received a placebo. In all treated patients, plaque index (PI), gingival index (GI) and gingival bleeding index (GBI) improved significantly, but with varying degrees of severity: while the combination of SRP and LrP had the greatest effect, the incidence of cancer decreased Combination SRP plus placebo even worse off than treatment only by LrP. Pocket depth and clinical attachment level were reduced by SRP plus LrP from 5,08 to 3,78 mm and 3,93 to 2,85 mm, respectively.
The meta-analysis by Martin Cabezas et al. [3] confirms the above results significantly. In comparison to SRP alone, the probiotic treatment provided a clearly improved therapeutic success.
Further study results with different risk groups confirm the successful use of LrP.
[1] Teughels et al. (J Clin Periodontol) 2013, 1025–35
[2] Vivekananda, et al. (J Oral Microbiology 2010, 2; 5344-ff)
[3] Rodrigo Martin-Cabezas, et al. (J of Clinical Periodontology) 2016; 520-530
Related Articles
-
Periodontitis and Its Impact on Our Patients’ Lives Learn with Prof. Filippo Graziani how periodontitis impacts quality of life, including physical, psychological, and social effects for dental professionals.
-
Stress and Oral Health: Implications of Chronic Stress As mounting evidence points to chronic stress as a clear risk indicator for periodontal disease, dental professionals should get proactive in addressing it.

-
Helping Patients Understand Holistic Oral and Body Health Today’s patients educate themselves on preventive care. Holistic care is an opportunity to improve not only oral health, but total-body health.

-
Experts Speak on Oral Cancer Challenges in Home Dental Care Prof. Carlo Lajolo and Ms. Susan Cotten join Sunstar Global to discuss oral health risks that result from cancer therapies and how to best support patients.

-
Ulcerative Oral Mucosa Lesions: Manifestations and Categories Oral mucosal lesions (aphthous ulcers) are acute, painful, whitish-yellow, fibrinous mucosal defects a with red halo. Here described their classification.

-
The Value of Saving Teeth vs. Dental Implants The value of saving teeth goes beyond dollars and cents. Regeneration paves the way for patient trust and better oral care opportunities.

-
Root Caries: Helping Patients Understand and Manage Helping patients understand what root caries are, and how to prevent them, is increasingly vital for dental pros as the global elderly population grows.

-
Lactobacillus reuteri Prodentis, Probiotic for Maintenance of Healthy Gums Multiple studies confirm that Lactobacillus reuteri Prodentis contained in GUM PerioBalance has plaque inhibition, anti-inflammatory, and antimicrobial effects.
-
New EFP Guidelines for Stage IV Periodontitis The EFP recently released evidence-based, interdisciplinary guidelines for treating stage IV periodontitis. Here’s what professionals should know.

-
Chlorhexidine, the Gold Standard in Dentistry, Mode of Action Chlorhexidine is one of the main antibacterial ingredients in oral care products as GUM® PAROEX®, its antibacterial activity can last for more than twelve hours.

-
How to Motivate your Patients to Use Interdentals It may be difficult for the patient to change habitual behaviors and implement your recommendations immediately. Discover how.

-
Delivering Innovative Oral Care for Your Dental Patients How can dental professionals take advantage of the latest technology, research, and best practices to provide cutting-edge service for their patients?

-
Interdental Cleaning, Extremely Important, but Still Underestimated Interdental cleaning is important. It's proven that rubber interdental cleaners, such as GUM® SOFT-PICKS®, provide optimal cleaning and increased compliance.
